
Full Mouth Dental Implants in Washington, DC
Full arch tooth replacement with All-on-4 and All-on-6 implants. Precision-placed by a specialist prosthodontist in Washington DC. Financing available.
Bring Your Smile Back to Life
A Complete Transformation: Are Dental Implants a Good Investment?
How long has it been since you felt truly confident smiling? Ate more than a soft food diet? Didn’t feel oral pain or discomfort? Suffering from many failing or missing teeth can take both a physical and emotional toll on you.
We understand how difficult it is to live every day without a complete and attractive smile that functions comfortably. We can help put an end to your painful and discouraging symptoms with full mouth solutions that fit your lifestyle, smile goals and budget!
From dentures to full mouth dental implants in Washington, D.C., our prestigious team at Elite Prosthetic Dentistry provides you with a treatment plan personalized to what you want, with an outcome that truly transforms your life by improving your function, health and confidence.
Consider Your Options
We’re pleased to offer three solutions for replacing all your failing or missing teeth: dentures, implant supported dentures and full mouth dental implants.
Dentures, though they seem like the most affordable option initially, aren’t a long-term solution, and over time, they may cause more problems than they solve. Implant supported dentures are dentures attached to dental implants that provide greater stability and function. Full mouth dental implants are the ultimate in full arch rehabilitation, permanently replacing all your failing or missing teeth with a fixed bridge of teeth attached to four or more dental implants.
While dentures seem like the “quick fix” for missing teeth, it’s important to know that healthier and more durable long-term solutions exist! Our cosmetic and implant dentist in Washington, D.C. is specifically trained in providing dental implants, and has years of experience placing and restoring this meaningful solution.
We invite you to learn about the process of receiving dental implants, the long-lasting, functional and healthy alternative to removable dentures.

Traditional Dentures
Removable Last 5+ years May require adhesives Allow bone recession Limit food choices
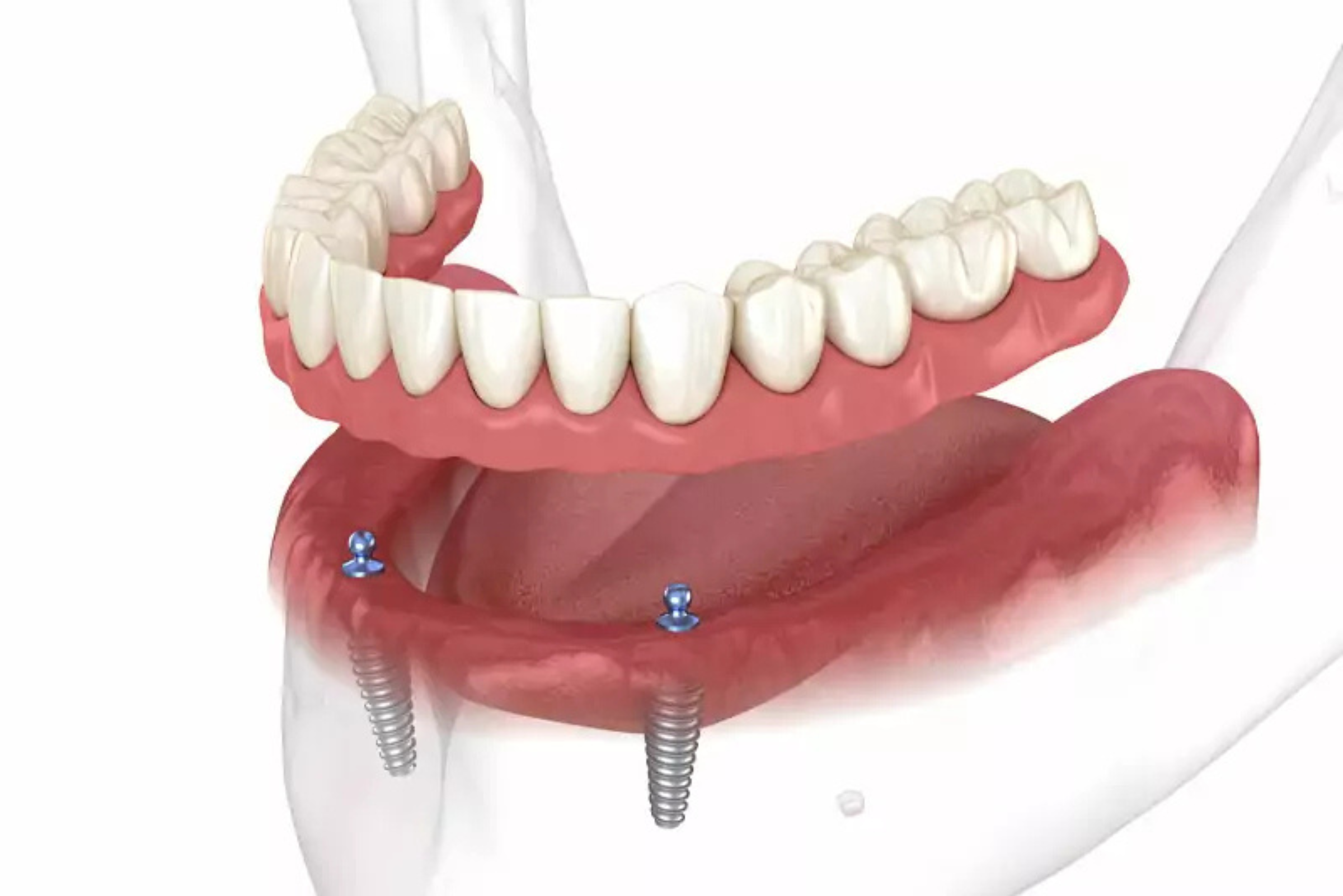
Implant Supported Dentures
Removable or fixed Last 10+ years Secured by 2+ implants Limit bone recession Expand food choices
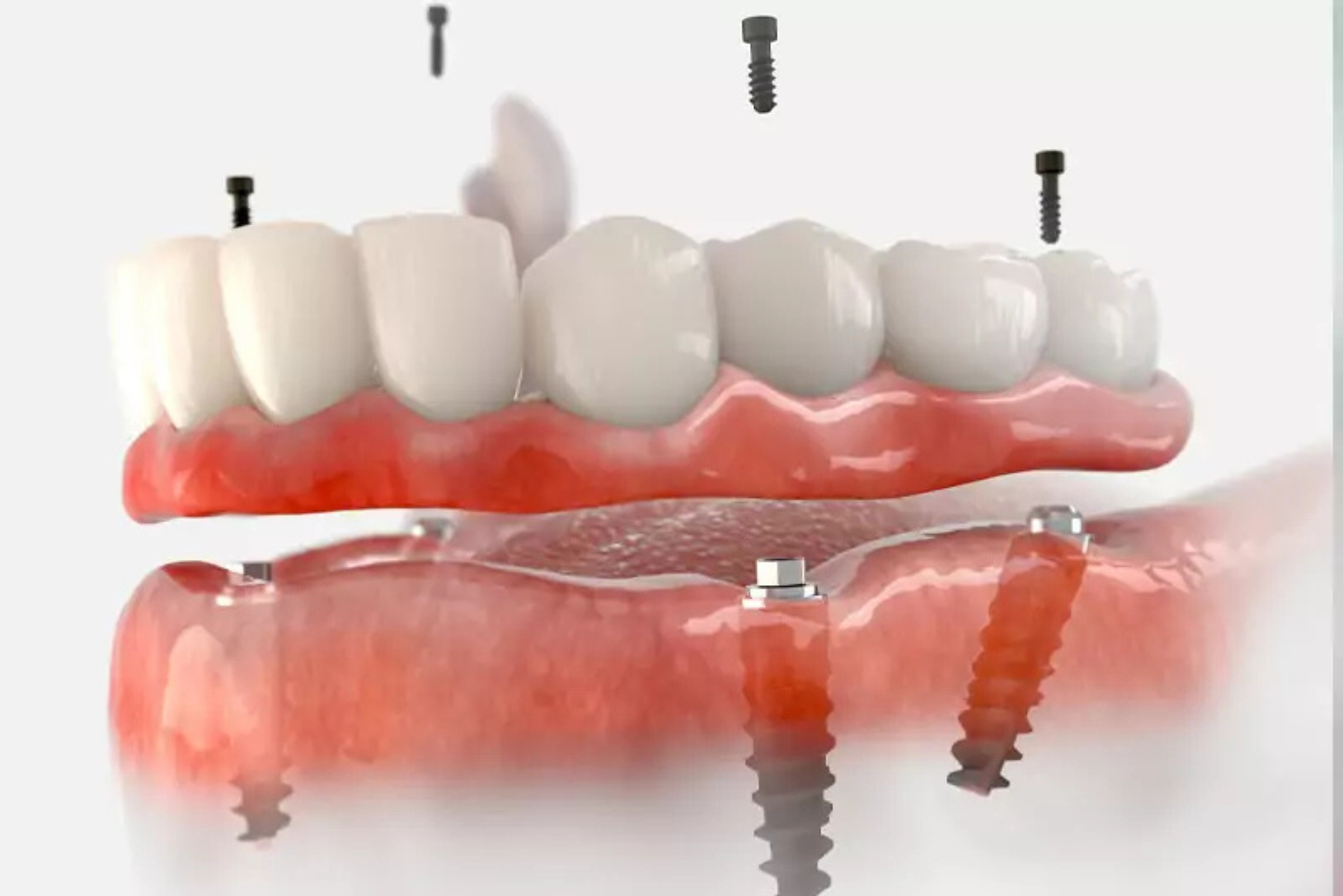
Full Mouth Dental Implants
Fixed for lasting support Last decades to a lifetime Secured by 4+ implants Prevent bone recession No dietary limitations
Our Smile Transformation Process
Step 1: Personalized Consultation
During your personalized consultation, you’ll be able to discuss your particular needs, smile goals and concerns, as well as any health conditions and issues we should consider. We may capture imaging, frequently from a cone-beam computed tomography (CBCT) scanner, to help us determine your candidacy for each tooth replacement solution.
Most patients who come to us are already candidates for full mouth dental implants, but if you have bone loss or gum disease, we will recommend receiving appropriate preliminary treatments.
Together we’ll discuss the best option for you and if you’d like, you can see before and after case studies from real Elite Prosthetic Dentistry patients, including how their treatment truly changed their lives. Dental implant pricing, insurance coverage and financing options will also be discussed.
If dental implants are best for you, our Washington, D.C. implant dentist completes precise surgical planning to ensure each implant placed is in the exact location, angle and depth for optimal lasting success and ideal esthetics.
Step 2: Precise Dental Implant Placement & Restoration
On the day of your surgery, you’ll check in at our front desk before being taken to your private suite. We offer sedation dentistry solutions to ensure that you feel relaxed throughout your visit.
Our patients typically report only minor discomfort, if any. Once you’re comfortable, we’ll place four or more dental implants into predetermined locations in your jawbone. We consider it our responsibility to ensure your implant is placed as accurately and successfully as possible, so it can last as long as possible. Whether you need one arch or a full mouth of new teeth, your entire surgical phase can be completed in just one day.
If you qualify, as many of our patients do, we can also immediately place your temporary teeth, which function and look just like natural teeth. You’ll never go a single day without a complete smile again!
Step 3: Final Restorations and New Beginnings
Your treatment site will need three or more months to fully heal after implant surgery. During this time, your dental implants will fuse with the jawbone in a process called osseointegration. It’s this bond that gives dental implants the stability and function they’re known for. After healing, you’ll return to our office to receive your final restorations.
The quality of restorations out there can vary. Focused on both function and esthetics, Elite Prosthetic Dentistry offers some of the most natural-looking options on the market today, able to match the look of natural teeth almost exactly, while also offering durable function. We’ll fit your custom-made bridge of new teeth to your dental implants, making sure your bite is properly aligned. You’ll leave our office with a lifelike, functional and confident new look that will last for years to come!
The All-on-4 Solution
The All-on-4® technique revolutionized full mouth implant restoration by allowing for a fixed bridge of teeth supported by just four strategically positioned implants. This approach is particularly beneficial for patients with limited bone in the posterior regions of the jaw. By angling the rear implants, Dr. Marlin can often avoid the need for bone grafting in cases where height or width would otherwise be insufficient.
The All-on-4® approach offers several advantages. Surgery is typically completed in a single visit. Temporary teeth can often be placed immediately after implant surgery, so you never go without a complete smile. The four-implant design distributes your bite forces effectively across your jawbone, creating long-term stability. And if cost is a consideration, All-on-4 can be more economical than traditional full mouth implants requiring six or more implants.
The All-on-6 and Beyond
For patients with adequate bone structure or those seeking maximum stability, Dr. Marlin may recommend an All-on-6® approach, using six or even eight implants to support the fixed restoration. Additional implants provide redundancy, improved load distribution, and can create a more natural-looking tooth position and angulation. This approach is ideal for patients with higher bite forces or those who want maximum longevity and security. See our All-on-4 vs. All-on-6 comparison for more detail.
The number of implants recommended depends on your bone quality and quantity, your bite force, your treatment goals, and Dr. Marlin’s assessment of what will provide optimal long-term success. These factors are thoroughly discussed during your consultation.
Living with Full Mouth Implants
Life after full mouth implant restoration is remarkably normal. Your fixed bridge functions like your natural teeth, with no removal required for cleaning or sleeping. You can eat whatever foods you enjoy without restrictions. Speaking is natural and clear, unlike with removable dentures that may shift or click. Oral hygiene involves regular brushing and flossing, just like natural teeth, though you may benefit from special floss threaders or water irrigation devices to clean around the implant posts.
Maintenance visits are essential. You’ll need periodic professional cleanings and examinations to ensure the health of your gums and bone around the implants. Regular radiographs help Dr. Marlin monitor bone levels and overall implant status. With proper care, full mouth implants can last for decades with proper care, making them one of the most cost-effective solutions when the total years of benefit are calculated.
Full Mouth Reconstruction: Beyond Replacement
For some patients, full mouth reconstruction means not just replacing missing teeth, but also addressing worn, damaged, or fractured teeth that remain. Dr. Marlin may recommend extracting heavily compromised natural teeth and replacing them with implants, creating a fully restored arch of beautiful, functional teeth. For patients seeking comprehensive rehabilitation that also addresses remaining teeth, a full mouth reconstruction may be the ideal path. This comprehensive approach can address longstanding bite problems, improve speech, restore proper facial height, and create a smile that looks and feels like the teeth you were meant to have.
Reconstruction cases are often complex and benefit significantly from Dr. Marlin’s expertise as a prosthodontist. He considers the relationship between all components of your smile, your jaw joint function, your bite relationships, and the esthetic outcome. The result is often a meaningful transformation that extends far beyond simply replacing missing teeth.
Bone Quality and Implant Success
Bone quality is critically important to implant success. Dense bone with good blood supply tends to integrate with implants more reliably and quickly. Bone quantity, as assessed by CBCT imaging, determines where implants can be placed and how many may be necessary. In some cases, bone grafting procedures are performed before or during implant surgery to enhance bone volume and density.
Dr. Marlin’s extensive experience allows him to work with various bone conditions and knows how to maximize the potential of your available bone structure. Whether through angled implants, staged approaches, sinus augmentation, or ridge augmentation procedures, he has solutions for nearly every scenario, even severe bone loss.
The Psychological Transformation
Patients who undergo full mouth implant restoration often report profound changes beyond the physical. Many have lived for years with failing or missing teeth, profoundly affecting their self-esteem and social interactions. The restoration of a complete, beautiful, functional smile frequently results in increased confidence, improved social engagement, and a measurable improvement in quality of life.
These psychological benefits are as important as the physical ones. Patients smile more readily, feel comfortable eating in social situations, and no longer experience the anxiety of dentures moving or becoming loose at an inappropriate moment. The peace of mind that comes with a permanent, secure restoration is invaluable to many of our patients.
Choosing Your Prosthodontist Partner
Full mouth rehabilitation is one of the most significant investments you can make in your oral health. Choosing the right prosthodontist to guide you through this journey is crucial. Dr. Gerald Marlin has decades of experience, has completed thousands of implant cases, and maintains relationships with referring dentists across the region due to his reputation for excellence and reliability.
When you choose Dr. Marlin and Elite Prosthetic Dentistry, you’re choosing not just a surgeon, but a restorative artist who understands that your smile is intimately connected to your identity and your confidence. We’re committed to understanding your needs, respecting your concerns, and delivering results that exceed your expectations.
Top 5 Mistakes People Make With Dental Implants

Do you have all the information you need to make the right decisions about dental implants? Don’t make any of these five common mistakes. Our exclusive checklist will steer you in the right direction.
Frequently Asked Questions
How long does the entire implant process take?
From initial implant placement to delivery of final restorations typically takes three to six months, depending on bone healing and the complexity of your case. In some cases, temporary teeth can be placed immediately after surgery.
Will I be able to eat normally after getting full mouth implants?
Yes. Once your restorations are complete and fully healed, you can eat virtually any food you enjoy, unlike with removable dentures that may limit your diet.
How often will I need to see the dentist after implant placement?
We recommend professional cleanings and examinations at least twice per year, more frequently if recommended by Dr. Marlin based on your specific situation.
What happens if I lose an implant?
While rare, if an implant fails to integrate, Dr. Marlin can place a new one after appropriate healing time. The fixed bridge design often allows continued function even if one implant requires replacement.
Can implants be placed if I have gum disease?
Gum disease must be treated before implant placement. Dr. Marlin will recommend appropriate periodontal therapy to ensure the best foundation for your implants.
Related Resources
- Sick of dentures or failing teeth?
- Browse patient success stories
- Read patient reviews
- View our smile gallery
Serving Patients From
Maryland
Bethesda | Cabin John | Chevy Chase | Kensington | North Bethesda | Potomac | Rockville | Silver Spring
Washington, DC
Cleveland Park | Dupont Circle | Foxhall | Georgetown | Kalorama | Palisades | Spring Valley | Tenleytown | Woodley Park
Virginia
Arlington | Fairfax | Falls Church | Great Falls | McLean | Oakton | Tysons | Vienna
Your Best Smile Is Within Reach
Request a specialist consultation with Dr. Marlin to discuss your situation and the most appropriate path forward.
Frequently Asked Questions
What is the difference between full mouth dental implants and All-on-4 or All-on-6?
Full mouth dental implants is the broader category that includes any approach to restoring an entire arch of teeth with implants. All-on-4 and All-on-6 are specific protocols within that category. All-on-4 uses four implants per arch with the rear implants angled to maximize available bone. All-on-6 uses six implants for broader force distribution and biomechanical redundancy. A full mouth case may also use eight or more implants in patients with adequate bone or specific functional demands. The right protocol depends on bone volume, bite forces, and long-term goals. See [All-on-4 vs. All-on-6](/all-on-4-vs-all-on-6/) for the clinical comparison.
How much do full mouth dental implants cost in Washington, DC?
Full mouth implant cost varies meaningfully based on the protocol selected (All-on-4, All-on-6, or a custom configuration), the prosthesis material (acrylic, zirconia, or porcelain-fused-to-zirconia), whether bone grafting or sinus augmentation is required, and whether one or both arches are being treated. A specialist consultation with CBCT 3D imaging produces a defined, itemized treatment plan rather than a generic price quote. Financing options are reviewed during consultation, and partial dental-insurance benefits often apply to portions of the case.
How long does full mouth implant treatment take from start to finish?
A straightforward full mouth implant case typically takes 6 to 9 months from the surgical placement to the final prosthesis. Patients often leave the surgical appointment with a temporary fixed prosthesis on the same day, then return for follow-up appointments during osseointegration, and receive the final laboratory-fabricated prosthesis once the implants have integrated with the bone. Complex cases involving bone grafting, sinus augmentation, or staged extractions may extend the timeline. The in-house lab eliminates the multi-week shipping delays typical of practices that send cases to external laboratories.
Will I have teeth during the healing period?
In most cases, yes. Immediate-load full-arch protocols allow placement of a temporary fixed prosthesis on the same day as implant surgery. The temporary lets patients eat, speak, and appear in public throughout the 3-to-6-month osseointegration period before the final prosthesis is fabricated. The temporary is intentionally designed for function during healing; the final prosthesis, designed and fabricated in the in-house lab, is what carries the long-term esthetic and biomechanical refinement.
How long do full mouth dental implants last?
Properly planned, placed, and maintained full mouth implants are designed to last for decades. Dr. Marlin's in-practice success rate exceeds 97% at 20-year follow-up across more than 3,900 implants placed, including full-arch cases. The prosthesis itself (the visible teeth) has a separate service life that depends on the material chosen: acrylic prostheses typically need refurbishment or replacement at 5 to 10 years, while zirconia prostheses commonly last 15 to 20 years or longer. The underlying implants, when well-cared-for, typically outlast multiple prosthesis cycles.
Am I a candidate for full mouth dental implants?
Most adults missing multiple teeth or with failing dentition are candidates for some form of full mouth implant treatment. Candidacy depends on bone volume, overall health, medications, smoking status, ability to attend follow-up visits, and commitment to home care. Patients who were told they were not candidates elsewhere often qualify under a specialist evaluation that considers bone grafting, sinus augmentation, ridge augmentation, or angled-implant approaches. A CBCT 3D scan during consultation defines what is actually possible for a given patient's anatomy.
What happens if a full mouth implant fails?
Implant failure is uncommon when cases are properly planned and maintained, but it is not impossible. A single failed implant in a full-arch case can often be replaced without disrupting the rest of the prosthesis, particularly with All-on-6 and higher-implant-count protocols where the redundancy is built into the original plan. Dr. Marlin has extensive experience with implant salvage and revision, including patients whose full-arch reconstruction was originally placed by another practice. See [Repairing Failing Implants](/repairing-failing-implants/) for revision options.
Why choose a prosthodontist instead of a corporate implant center for full-arch treatment?
Corporate implant centers operate on a high-volume, production-line model with rotating providers across surgical and restorative phases. Specialist prosthodontic practice is structurally different: the same doctor plans the case, performs the surgery, designs the final prosthesis, and provides long-term follow-up. The prosthesis is fabricated in an in-house lab where the master ceramist works directly with Dr. Marlin, rather than being shipped to an external production facility. For a treatment of this complexity and cost, single-doctor continuity and direct lab control have measurable effects on the long-term outcome. See [Specialist vs. Implant Centers](/specialist-vs-implant-centers/) for the detailed comparison.
Related Patient Success Stories
Explore similar patient success stories demonstrating our expertise in advanced prosthetic dentistry.
 Before
Before  After
After How Older Implant Crowns Were Redesigned for a Better Bite and More Natural Appearance
The patient came in after years of living with implant-supported crowns placed more than twenty years earlier that no longer looked or functioned well. CBCT evaluation, reviewed with a radiologist colleague, showed the implants had been placed too far to the buccal in very thin bone and could not support a healthy long-term restoration.
 Before
Before  After
After How a Front Tooth Lost to Childhood Trauma Was Rebuilt with Bone Grafting and a Long-Lasting Implant
A teenager was referred by her father after earlier trauma left her upper left front tooth slowly failing from root resorption. She was still growing, so an immediate implant was the wrong move. The tooth had to be maintained to buy time, then replaced correctly once she reached skeletal maturity.
 Before
Before  After
After How Severe Bone Loss and Bite Dysfunction Were Rebuilt with All-on-6 Implants and a Milled Zirconia Hybrid Prosthesis
The patient presented with severe bone loss, advanced periodontal disease, malocclusion, and a dysfunctional bite that required full-arch rebuilding.
 Before
Before  After
After Implant Supported Reconstruction: Failing Bridgework and Missing Back Teeth Rebuilt with Coordinated Specialist Care
Referred by another dental specialist with severe bone resorption on the upper left, multiple broken-down lower teeth requiring extraction, and failing lower back teeth that had left the bite without solid support. No single procedure, and no single provider working alone, could rebuild a situation this interconnected.
 Before
Before  After
After How Worn Teeth Were Rebuilt for a Natural, Stable, Long-Lasting Smile
Decades of gradual wear had shortened, flattened, and darkened the teeth, changing the smile and quietly affecting the bite. The patient was not in crisis but wanted the dentistry planned and done correctly, with tooth proportions, esthetics, and bite stability handled as one system rather than patched a piece at a time.
 Before
Before  After
After Severe Restorative Breakdown Rebuilt with a Coordinated Full-Mouth Reconstruction
Multiple older restorations placed at different times over many years, broken-down teeth, a significant malocclusion, an asymmetrical smile, and two upper front teeth that could no longer be saved. No single repair could address a pattern this widespread.
Related Articles
Deepen your knowledge with additional insights on this topic.
 Dental Implants
Dental Implants If a Single Front Tooth Is Replaced with an Implant, Can It Look Natural?
Yes. See the four steps, with real case photos, that make a single front tooth implant indistinguishable from the natural tooth beside it. Washington, DC.
 Dental Implants
Dental Implants What Is Precision Implant Placement (PIP)?
Precision Implant Placement plans each implant virtually on a CBCT scan, then delivers it with a custom surgical guide. See the three steps with real images.
 Dental Implants
Dental Implants What Is the Ideal Surgical Guide for Precision Implant Placement?
Not all surgical guides are equal. The gold standard is CBCT-based: planned virtually in 3D, 3D printed, and seated on your teeth. A DC prosthodontist explains.
 Dental Implants
Dental Implants When Should an Implant Not Be Done?
Healthy roots, thin bone, steep bony angles: a DC prosthodontist shows a real case where refusing implants was the right call, and what was done instead.
 Dental Implants
Dental Implants What Is Staged Implant Therapy?
Staged implant therapy replaces failing teeth in phases while you keep fixed teeth the entire time. A DC prosthodontist walks through a real case in stages.
Dental Implants The Four Types of Dental Implants: Which One Is Right for You?
Endosteal, subperiosteal, zygomatic, and mini implants each solve a different problem. A DC prosthodontist explains the four types and who each one fits.
Full Mouth Dental Implants in Washington, DC Near You
Dr. Marlin provides full mouth dental implants in washington, dc services to patients throughout the Washington, DC metropolitan area. Select your community to learn more.
Ready to Transform Your Smile?
With 40+ years of experience and 3,900+ dental implants placed and restored, Dr. Marlin delivers results that last. Request a specialist consultation.