How Aging Crowns and a Long-Standing Bridge Were Rebuilt with a Coordinated Restorative Plan
Older crown work and a long-standing bridge replaced before treatment became an emergency
Replacing aging crowns and a long-standing bridge in Washington, DC. This documented case at Elite Prosthetic Dentistry rebuilt older restorative work through a coordinated plan that combined replacement crown work, bridge replacement, provisional verification, in-house laboratory fabrication, and sedation-supported treatment. Treatment was planned and completed by Gerald Marlin, D.M.D., M.S.D., a prosthodontist focused on complex restorative dentistry, full mouth reconstruction, and long-term crown and bridge care.
Case at a Glance
- Treatment
- Coordinated restorative reconstruction with replacement crowns and bridge
- Approach
- Diagnostic workup, sequenced planning, provisional verification, in-house laboratory fabrication, post-treatment radiographic verification, and integrated comfort planning
The patient traveled from outside the Washington metropolitan area because he wanted older crown and bridge work evaluated before it became an emergency. He was preparing for a demanding professional schedule and wanted a predictable, natural-looking result completed through a carefully planned sequence rather than a last-minute repair.
Full-face view
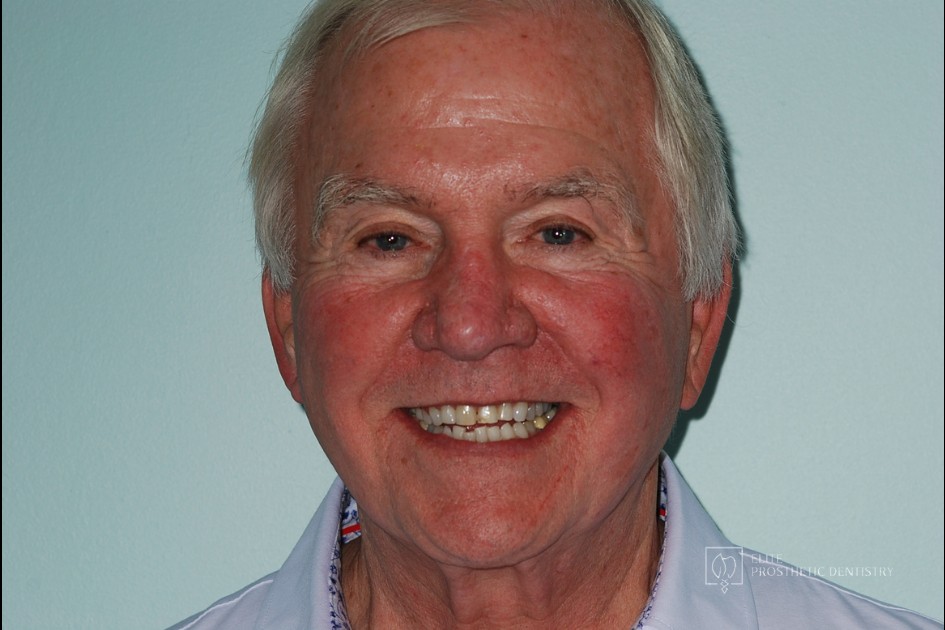 Before
Before
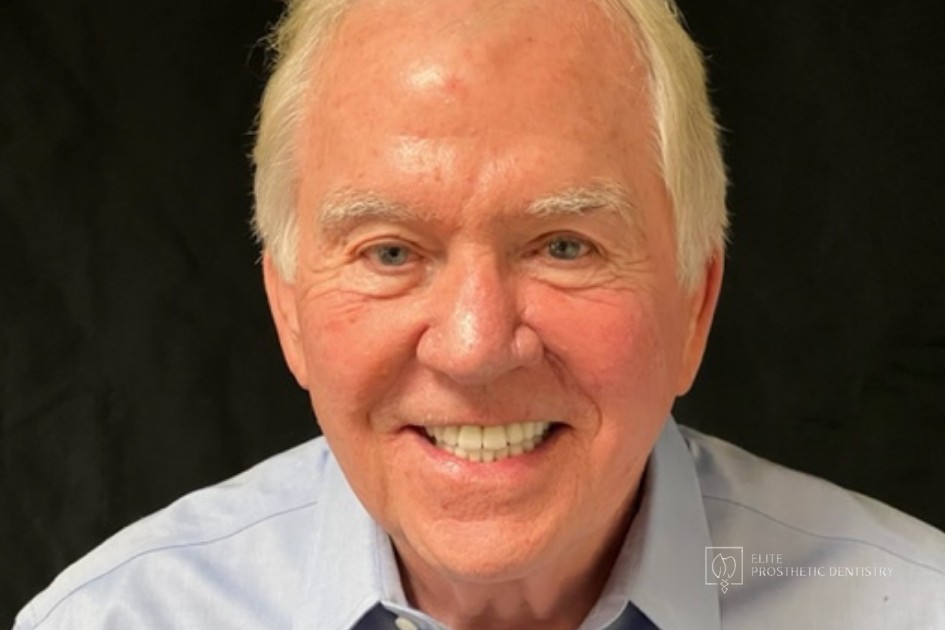 After
After
The presenting condition
The patient presented with crown work and a long-standing bridge that had aged together over many years. The restorations were not in sudden failure, but the pattern was clear: older dental work was approaching the point where conservative repair would no longer provide a predictable answer. The bridge was beginning to lose long-term reliability. The crowns showed margin changes, color shift, surface wear, and the kind of restorative aging commonly seen after many years of service. The lower anterior wear pattern also suggested that the bite needed to be considered as part of the plan, not treated as a separate issue.
Clinical Findings
- →Aging upper anterior crown work with margin changes, color shift, and surface wear
- →Long-standing bridge no longer providing predictable long-term function
- →Periodontal changes consistent with the age and history of the older restorative work
- →Occlusal wear pattern on the lower anterior teeth suggesting a bite relationship the original crown work had not fully addressed
- →Patient preference for treatment delivered with intravenous sedation integrated into the appointment sequence
Why this case required prosthodontic-level planning
This case was different from a routine crown or bridge replacement because the patient was not simply trying to repair one broken tooth. The crown work, bridge, periodontal tissues, esthetics, and bite had all aged together. Replacing only the most visible or most urgent section would have risked creating another short-term solution. The better approach was to evaluate the entire restorative pattern, confirm the planned result with provisionals, and then fabricate the final bridge and crowns only after the design had been tested in the patient’s own mouth. For patients who value quality and want dentistry done correctly, the most important decision is often not which crown or bridge is selected, but whether the periodontal foundation, prosthetic design, occlusal scheme, esthetics, and comfort plan are coordinated before treatment begins.
The treatment plan
-
1
Comprehensive diagnostic workup
Full diagnostic records including photographs, radiographs, and bite registration. The reconstruction sequence was mapped before restorative treatment began.
-
2
Sequenced multi-phase plan
Treatment was sequenced so that periodontal preparation, restorative preparation, provisionalization, and final delivery each had the foundation they needed. The plan was organized around predictability rather than speed.
-
3
Replacement of aging crown work
The aging crowns were replaced with new restorations designed to coordinate with the planned final occlusal scheme rather than as independent one-tooth events.
-
4
Replacement of the long-standing bridge
The older bridge was replaced with a new restoration coordinated to the rebuilt arch so that the bridge, surrounding crowns, and bite functioned as one system.
-
5
Provisional verification before final restorations
Provisional restorations were placed and worn long enough to verify the planned restorative endpoint in the patient's own mouth, under his own bite, before final fabrication.
-
6
Comfort planning integrated with the clinical sequence
Intravenous sedation was integrated into the appointment plan so longer restorative sessions could be completed comfortably without compromising the precision of the work.
Provisionalization: Progressive Bite Development and Aesthetic Correction
 Provisional
Provisional
 Provisional
Provisional
The outcome
The case moved from aging crown work and a long-standing bridge that had outlived predictable repair to a coordinated restorative result completed across a planned sequence. The new crowns and bridge were designed and delivered as one system. The bite, periodontal foundation, prosthetic design, and final esthetics were treated as a single case rather than as separate restorations. The final bridge and crowns were fabricated with direct coordination between Dr. Marlin and the practice’s in-house laboratory to maintain control over fit, contour, bite integration, and esthetics. The in-house arrangement, in continuous operation since 1985, allowed the prosthodontist and ceramist to refine contour, color, marginal fit, and incisal translucency together with the patient’s records on the bench.
Result Highlights
- ✓Aging crown work replaced with coordinated new restorations
- ✓Long-standing bridge replaced as part of one sequenced plan
- ✓Provisional restorations used to verify form, bite, and esthetics before final fabrication
- ✓Treatment delivered comfortably across the planned sequence with sedation integrated as needed
- ✓Final restorations fabricated under direct in-house laboratory coordination
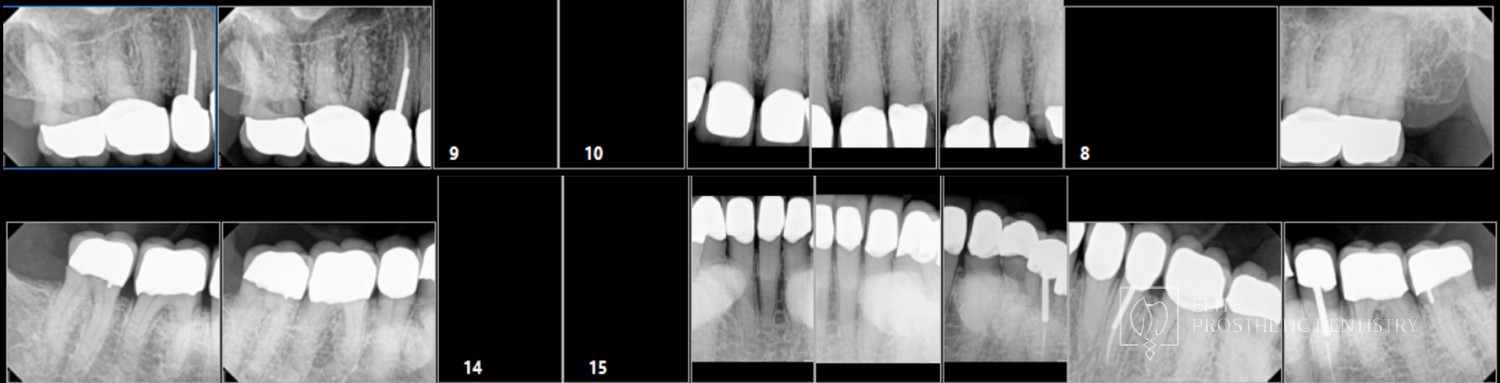
- ✓Post-treatment radiographic verification documented the fit and supporting structure
Close-up smile view
 Before
Before
 After
After
Additional intraoral view
 Before
Before
 After
After
Post-treatment radiographic series
Want older crown and bridge work evaluated before it becomes an emergency? A private consultation can map a coordinated plan on your own calendar.
Schedule a Private ConsultationWho this case may sound familiar to
This story tends to resonate with patients in a few recognizable situations:
- Your older crown work is showing margin changes, color change, or surface wear that makes you question how long it will last.
- Your long-standing bridge no longer feels fully predictable, and you would rather plan its replacement before it becomes an emergency.
- Your restorative work and periodontal condition have both aged, and you want them evaluated as one coordinated problem rather than as separate repairs.
- You prefer to complete longer or more complex restorative appointments with sedation support when appropriate.
- You want a coordinated plan, on your own calendar, rather than reactive treatment as each piece fails.
If any of those describe where you are, a consultation with Dr. Marlin can establish the diagnostic picture and the specific options for your case.
If your bridge is loose, your older crowns are changing, or you are beginning to question whether repeated repairs are still the right answer, a comprehensive evaluation can clarify what is happening and what a coordinated replacement plan would look like for your case.
Request a Comprehensive EvaluationFrequently asked questions
Why replace dental crowns that are not actively failing?
Older crown work often begins to show changes in groups rather than one tooth at a time, especially when the restorations were placed during the same period. Margin changes, color shift, gum recession at crown edges, and bite wear can all indicate that the restorations are approaching the end of their predictable service life. Replacing them through a planned sequence can reduce the risk of repeated emergency repairs and allows the final result to be designed as a coordinated system.
Can older crowns and a long-standing bridge be replaced together?
In many cases yes. When more than one area of older restorative work has aged together, replacing them as one coordinated plan can produce a more predictable long-term result than reacting to each restoration separately. The prosthodontist plans the final restorative endpoint first and sequences the replacement of each aging component to that endpoint.
How does a prosthodontist plan crown replacements differently?
A single crown can often be treated successfully as an individual restoration. When multiple crowns, bridges, bite relationships, and periodontal tissues are involved, prosthodontic planning focuses on how all of those components function together. The final endpoint is planned first, then each tooth, margin, contact, contour, and occlusal relationship is designed to support that endpoint.
Can crown design improve mildly misaligned or rotated teeth without orthodontics?
In selected clinical situations, yes. When the tooth positions, occlusion, and bone support allow it, crown design can sometimes improve minor rotations and positional discrepancies. This requires careful three-dimensional planning and precise management of contour and contacts. Where orthodontic correction is the better biological answer, that should be part of the discussion.
How is sedation handled for a multi-stage reconstruction?
When a patient prefers sedation for longer or more complex restorative appointments, it is integrated into the treatment plan as one element of the broader care sequence. It can allow precise work to be completed over longer continuous sessions while helping the patient remain comfortable.
Why does an in-house dental laboratory matter for cases like this?
Crown and bridge work is a collaboration between the prosthodontist and the ceramist. When the laboratory is in the same facility, the doctor and ceramist can refine contour, color, marginal fit, and incisal translucency together with the patient’s records immediately available. Elite Prosthetic Dentistry has operated an in-house dental laboratory continuously since 1985.
How is crown work verified after cementation?
Verification is a clinical step performed after the final restorations are cemented. It may include radiographic documentation of marginal integrity where the crown meets the tooth, review of soft-tissue response, and occlusal contact verification in centric and excursive movements.
How long should well-planned crown work be expected to last?
Crown longevity depends on the underlying tooth, restoration design, material selection, bite forces, fit, home care, and maintenance. Well-planned, well-fabricated crowns supported by sound tooth structure and a properly distributed occlusion can function for many years. Many Elite Prosthetic Dentistry restorations have remained in service for more than 35 years.
More about the work behind this case
This case sits at the intersection of replacing aging dentistry, full mouth reconstruction, custom dental crowns, dental bridges, natural aesthetic rehabilitation, and sedation-supported restorative care. The diagnostic depth, provisional verification, post-treatment radiographic review, and in-house laboratory control are part of the practice philosophy that supports cases of this complexity. Elite Prosthetic Dentistry treats patients from across the DMV including Bethesda, Chevy Chase, McLean, Arlington, Potomac, and Great Falls, and from out-of-area markets including Richmond, Virginia.
Related Services
About the Provider
This case was treated by Gerald M. Marlin, D.M.D., M.S.D., at Elite Prosthetic Dentistry in Washington, DC. Dr. Marlin is a specialty-trained prosthodontist with more than 40 years in clinical practice, more than 3,900 implants placed and restored, and 9 U.S. patents in implant restoration. Elite Prosthetic Dentistry has operated a continuous in-house dental laboratory since 1985.
4400 Jenifer Street NW, Suite 220, Washington, DC 20015 | (202) 244-2101
Related Patient Success Stories
Explore similar patient success stories demonstrating our expertise in advanced prosthetic dentistry.
 Before
Before  After
After How Older Implant Crowns Were Redesigned for a Better Bite and More Natural Appearance
The patient came in after years of living with implant-supported crowns placed more than twenty years earlier that no longer looked or functioned well. CBCT evaluation, reviewed with a radiologist colleague, showed the implants had been placed too far to the buccal in very thin bone and could not support a healthy long-term restoration.
 Before
Before  After
After How Severe Bone Loss and Bite Dysfunction Were Rebuilt with All-on-6 Implants and a Milled Zirconia Hybrid Prosthesis
The patient presented with severe bone loss, advanced periodontal disease, malocclusion, and a dysfunctional bite that required full-arch rebuilding.
 Before
Before  After
After Implant Supported Reconstruction: Failing Bridgework and Missing Back Teeth Rebuilt with Coordinated Specialist Care
Referred by another dental specialist with severe bone resorption on the upper left, multiple broken-down lower teeth requiring extraction, and failing lower back teeth that had left the bite without solid support. No single procedure, and no single provider working alone, could rebuild a situation this interconnected.