
Loose Dental Implant in Potomac, MD
Implant loosening from bone loss or failed osseointegration. Dr. Marlin diagnoses why implants fail to integrate. Potomac implant specialists.
Loose Dental Implant From Bone Loss and Failed Osseointegration in Potomac, MD
Some loose implants represent a failure that occurred at the very moment of surgical placement: the implant never achieved stable biological attachment to bone. This failure of osseointegration is distinct from bone loss around an initially successful implant. At Elite Prosthetic Dentistry, we distinguish these scenarios through careful diagnostic evaluation, understand the underlying causes, and develop appropriate treatment strategies that address the actual problem rather than just the symptom.
Understanding Osseointegration: The Foundation of Implant Success
Osseointegration is the biological process where living bone fuses directly to the titanium implant surface. Without osseointegration, an implant is merely a foreign body in your mouth, held in place only by mechanical friction and soft tissues. True stability requires bone fusion. Understanding this process is critical when evaluating failed implant integration or bone loss around implants.
The Biological Process
When an implant is placed, bone around the fixture is disturbed by the surgical procedure. Over the first weeks and months, bone healing occurs in phases. Initially, inflammatory cells clean up the surgical wound. Then, osteoblasts (bone-forming cells) begin to deposit new bone. This new bone gradually grows closer to the implant surface. Advanced techniques like precision implant placement optimize conditions for osseointegration.
Titanium is biocompatible and doesn’t trigger a rejection response. The body treats it as a non-threatening foreign material. Instead of building a barrier of scar tissue around the implant (as happens with incompatible materials), bone directly grows toward and contacts the titanium surface.
Over 3-6 months, enough bone fuses to the implant surface that the fixture becomes immobile. We say the implant is “osseointegrated.” At this point, the implant can bear load and function as a tooth root.
The Critical Healing Period
The first weeks after implant placement are critical. During this time, the implant must remain undisturbed while bone heals. Any condition that disrupts bone healing can prevent or delay osseointegration. This is why precision implant placement and careful post-operative management are essential components of implant dentistry. Patients should avoid overloading during this period.
Why Osseointegration Fails
Multiple factors can prevent or delay osseointegration, creating a loose implant that never achieves proper stability.
Infection at the Implant Site
The Problem
If bacteria contaminate the implant site during surgery or in the immediate post-operative period, infection develops. Bacterial toxins trigger inflammation, and inflammatory cells destroy bone tissue and prevent healing. The implant cannot osseointegrate in an infected site because bone formation cannot proceed against active infection.
Clinical Presentation
An infected implant site may show redness, swelling, drainage, or pain. Some infections are mild and asymptomatic initially. By the time you notice the implant is loose, significant infection damage may have occurred.
Prevention and Treatment
We use sterile surgical technique and prescription antibiotics post-operatively to prevent infection. If infection occurs, we treat aggressively with additional antibiotics and sometimes surgical intervention to clean the site.
Excessive Heat During Surgical Drilling
The Problem
Bone is living tissue. When surgical drills cut bone, friction creates heat. If drilling speed is too fast or if improper technique is used, bone temperature can exceed critical thresholds. Bone cells die from heat damage (thermal necrosis). Dead bone cannot support osseointegration.
Modern Prevention
Modern surgical technique using cooled drilling with proper speed and irrigation prevents thermal damage. However, older drilling techniques or high-speed drilling without cooling created this problem historically.
Diagnosis
Thermal necrosis from surgery is difficult to distinguish from other causes of failed integration without surgical exploration. Radiographs might show gap between bone and implant, but bone loss alone doesn’t confirm thermal damage.
Immediate Loading Before Healing
The Problem
The healing process takes time. If an implant is loaded (forces applied through the crown) before bone has fused, movement occurs at the bone-implant interface. This movement disrupts bone healing and prevents osseointegration.
Traditional implant protocols recommend waiting 3-6 months after placement before placing the final crown. Some modern immediate-load protocols reduce this timeline but still respect the biology of healing.
Risk Factors
Immediate loading carries higher failure risk than delayed loading. Some cases succeed with immediate loading, but the biological safety margin is reduced. Patients with poor bone quality, compromised healing, or medical conditions increasing infection risk are poor candidates for immediate loading.
Prevention
We follow evidence-based loading protocols. For most patients with typical bone quality, we recommend waiting 4-6 months after implant placement before final crown restoration. We communicate this timeline clearly so patients understand the reason.
Smoking
The Impact
Smoking impairs bone healing dramatically. Nicotine constricts blood vessels, reducing blood supply to the implant site. Reduced blood supply means reduced oxygen delivery and reduced delivery of bone-forming cells. Smoking also impairs immune function, increasing infection risk.
Smokers have roughly double the implant failure rate of non-smokers. This is not a modest difference. This is a major risk factor.
How We Address It
We counsel all patients about smoking before implant placement. For active smokers, we strongly recommend smoking cessation before surgery. Some surgeons will not place implants in active smokers because the failure risk is unacceptably high.
If you’ve quit smoking recently, healing is still improved. Even smoking reduction without complete cessation improves outcomes.
Uncontrolled Diabetes
The Impact
Diabetes impairs bone healing and increases infection risk. High blood glucose levels suppress immune function and reduce the ability of bone-forming cells to function. Diabetic patients with poor blood sugar control have significantly higher implant failure rates.
Optimization Before Surgery
We recommend that diabetic patients optimize their blood sugar control before implant placement. Working with your primary care physician to achieve a hemoglobin A1c below 7 percent before surgery significantly improves healing and reduces failure risk.
Post-Operative Management
We monitor diabetic patients more closely post-operatively and maintain more conservative loading timelines.
Medications That Impair Healing
Certain medications suppress bone healing or immune function.
Bisphosphonates, medications used to treat osteoporosis and prevent metastatic cancer bone disease, can impair bone healing and increase the risk of implant failure. Patients on long-term bisphosphonate therapy require careful surgical planning.
Steroids, whether taken systemically or topically for long periods, impair healing. Even inhaled steroids for asthma, if used chronically, can slightly increase implant risk.
Immunosuppressive medications, used in transplant patients or to treat autoimmune diseases, directly reduce immune function and infection-fighting ability.
We review all medications before implant surgery and discuss specific risks and modifications as needed.
Radiation Therapy History
The Impact
Patients who have undergone head or neck radiation for cancer treatment often have severely compromised bone healing capacity. Radiation damages bone-forming cells and reduces blood supply to bone. Implants placed in previously radiated bone have much higher failure rates.
Timing Considerations
We recommend waiting at least 6-12 months after radiation therapy before placing implants, allowing maximum bone recovery. We often recommend bone grafting to improve bone quality and increase implant success likelihood.
Surgical Modifications
For patients with radiation history, we modify our surgical approach, use longer healing periods, and monitor more closely for complications.
Poor Bone Quality
The Problem
Bone is not uniform. Some bone is dense and well-vascularized; other bone is sparse and poorly vascularized. Implant success is higher in dense bone with good blood supply.
Some patients have naturally poor bone quality from age, genetic factors, or medical conditions. Others develop poor bone quality from long-standing tooth loss (bone resorbs when teeth are missing).
Assessment
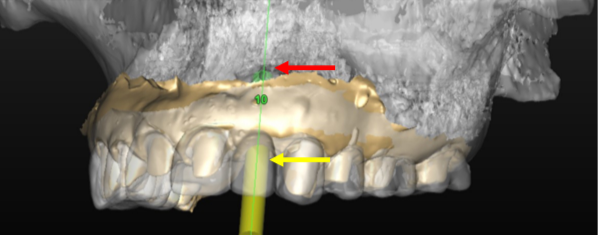
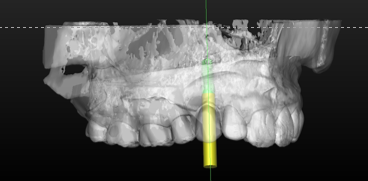
We evaluate bone quality and quantity before implant placement using radiography and CBCT imaging. Poor quality bone can sometimes be augmented with bone graft, improving implant success likelihood.
Bone Regeneration Disorders
Certain genetic and metabolic conditions affect bone formation and healing. These are rare but can cause implant failure despite otherwise appropriate surgery. Conditions like hypoparathyroidism, hypophosphatasia, or osteogenesis imperfecta affect bone biology directly.
Diagnosing Failed Osseointegration
Distinguishing a failure to integrate from other causes of loosening requires systematic evaluation.
Timeline Assessment
An implant placed several years ago that suddenly becomes loose has likely lost bone that was previously integrated. An implant placed months ago that never felt stable might never have integrated.
Radiographic Findings
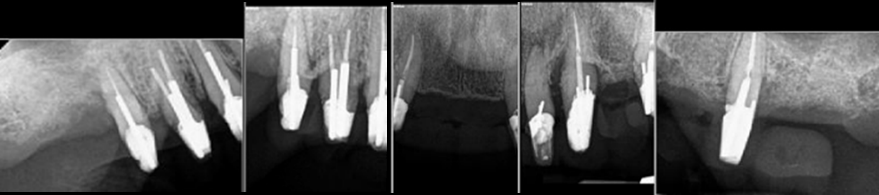
Radiographs show a gap or radiolucency between bone and implant surface when integration has failed. A halo around the implant indicating bone loss also suggests failed integration or subsequent bone loss.
Clinical Mobility
A fixture that has never integrated feels mobile in bone, moving freely when testing pressure is applied. A fixture that has integrated but lost bone support also feels mobile. The clinical feel is similar, but the diagnosis is clarified by radiographic history.
Surgical Exploration
In some cases, we surgically expose the implant to visually assess bone contact. If no bone contacts the fixture surface (naked implant), integration has failed. If bone contacts the fixture but appears minimal, partial integration or subsequent bone loss has occurred.
Treatment Strategies Based on Diagnosis
Once we’ve diagnosed failed osseointegration, treatment depends on the severity and cause.
Implant Removal and Investigation
If an implant has never integrated, removal is the appropriate treatment. We remove the fixture and investigate the bone site to understand what prevented integration. A culture of bone and tissue might reveal infection. Visual inspection reveals bone quality and any signs of thermal necrosis.
Addressing Modifiable Causes
If we identify a modifiable cause (smoking, poor diabetes control, infection), we address it before considering replacement.
Smoking: We engage patients in smoking cessation. Some patients cannot quit but can significantly reduce cigarette consumption. Any reduction improves healing prospects.
Diabetes: We coordinate with the patient’s physician to optimize blood sugar control.
Infection: We treat any residual infection before replacement implant placement.
Medication: We work with the patient’s physician to discuss whether alternatives to problematic medications are available.
Bone Grafting Before Replacement
After failed implant removal, the socket may have compromised bone quality. We sometimes perform bone grafting to regenerate bone and improve quality before replacement implant placement.
Bone graft materials (autografts from your own bone, allografts from donor bone, or synthetic substitutes) fill the socket and encourage bone regeneration. Over 4-6 months, new bone forms, improving implant site quality. This preparation maximizes your replacement implant’s chances for successful osseointegration.
Replacement Implant Placement With Modified Protocol
For replacement implants, we use a more conservative protocol than for the original implant.
We wait longer before loading (6 months instead of 4 months).
We modify surgical technique to be extra gentle.
We use extended healing time and avoid any premature loading.
We monitor more closely post-operatively.
These modifications reduce the risk that the replacement implant experiences the same fate as the original.
The Role of Patient Selection in Implant Success
Not every patient is an ideal implant candidate. Honest assessment of medical risk factors before treatment begins is essential.
High-Risk Patients
Some patients have multiple risk factors (smoker, diabetic, on bisphosphonates, radiation history) that compound failure risk. For these patients, we discuss alternatives to implants, including traditional fixed bridges or removable dentures. Sometimes implants are attempted despite high risk, but with clear communication about increased failure likelihood and need for modified protocols.
Optimization Before Surgery
We often recommend that high-risk patients optimize their health before surgery. Smoking cessation, diabetes control, medication review, and infection treatment all improve implant success likelihood.
Realistic Expectations
We communicate clearly about implant success rates for different patient populations. High-risk patients should understand that implants may fail despite appropriate treatment, and they need backup plans.
Potomac and Patient Health Optimization
Potomac residents tend to be engaged with preventive healthcare and willing to optimize their health before elective procedures. This mindset is ideal for implant patients, particularly those in higher-risk categories.
Our Potomac office location (12 minutes from central Potomac) is conveniently positioned to serve this population and facilitate the multiple consultations and evaluations that complex cases require.
Related Conditions and Comprehensive Care
Failed osseointegration or bone loss around implants sometimes involves related problems. Failed implant integration is a comprehensive overview of why osseointegration fails and treatment strategies. Dental implant bone loss describes the process of bone loss around implants and management strategies.
Bone grafting is frequently part of treating sites after failed implant removal and preparing for replacement. For Potomac patients, we offer dental implants for Potomac patients, bone grafting for Potomac, implant repair in Potomac, full mouth reconstruction in Potomac, implant denture repair in Potomac, sedation dentistry in Potomac, and full mouth dental implants in Potomac.
Repairing failing implants encompasses broader strategies for managing implants with multiple complications. Precision implant placement describes surgical planning and technique modifications that reduce risk of placement-related failures. Advanced restorative dentistry principles ensure your replacement restoration optimizes the biology of your healed implant site.
Dr. Marlin’s Approach to Failed Osseointegration
Dr. Marlin’s Master of Science degree in Prosthodontics includes advanced training in implant complications and failure modes. He has evaluated hundreds of failed implants and understands the biological and technical factors that contribute to failure.
He works closely with oral surgeons who specialize in complex bone grafting and implant salvage procedures. When your case requires surgical expertise, we facilitate collaboration that optimizes your outcomes.
Scheduling Your Evaluation
If your implant is loose and you suspect failed osseointegration or bone loss, bring any records from the original implant surgery, including radiographs and operative reports. These documents help us understand the original treatment plan and assess what has changed.
Request an appointment for comprehensive evaluation. We’ll assess your implant, review your medical history, take updated radiographs, and discuss realistic treatment options.
Read more about Dr. Marlin’s background and approach to complex implant cases.
Failed osseointegration is disappointing, but understanding the cause and addressing it in replacement implant therapy significantly improves success likelihood. Let us help you navigate this challenge and restore your smile.
Frequently Asked Questions
What causes an implant to fail to integrate with bone in the first place?
Multiple factors can prevent osseointegration: infection at the implant site, excessive heat during surgical drilling, immediate loading before healing is complete, smoking, uncontrolled diabetes, certain medications, poor bone quality, radiation therapy, or bone regeneration disorders. The cause determines what interventions might help.
Can a loose implant from failed integration be saved, or does it always need removal?
If the implant never integrated (never fused to bone), it cannot be saved because there's nothing to save. The fixture is essentially floating. Removal is necessary. However, determining whether failed integration occurred at placement or whether integration occurred then later was lost requires careful diagnostic evaluation.
Are there medical conditions that guarantee implant failure?
Some conditions increase risk significantly but don't guarantee failure. Uncontrolled diabetes, immunosuppression, radiation therapy, and certain bone diseases increase failure risk. With careful patient management, implants can succeed even in these populations, but risk is higher than in healthy patients.
If my first implant failed to integrate, will a replacement implant fail too?
Not necessarily. We investigate why the first implant failed and modify our approach for replacement. If the cause was modifiable (smoking, infection, diabetes control), addressing it dramatically improves second implant success. If the cause was non-modifiable (radiation therapy), we might recommend alternatives to implants.
How is failed integration different from bone loss around a previously integrated implant?
Failed integration means the implant never achieved stable bone contact. Bone loss around an integrated implant means the implant fused initially but bone was subsequently lost. These require different diagnostic approaches and different treatments.
Related Patient Success Stories
Explore similar patient success stories demonstrating our expertise in advanced prosthetic dentistry.

Temporary Crowns Restore Patient's Smile in Just One Day with an Immediate Smile Makeover
A patient from Potomac, Maryland, came to Elite Prosthetic Dentistry with the chief complaint of pain from a failing dental implant and its significant impact on her appearance.

Multi-Faceted Treatment for Patient Unhappy With Her Artificial-Looking Crowns, Teeth and Gums
Many patients come to Elite Prosthetic Dentistry unhappy with the appearance of their smile. However, this particular patient presented with multiple interconnected problems that together created a smile she found deeply unsatisfying.

Treating Kevin’s Collapsed Bite with a Complete Smile Makeover with New Dentures
Dentures are sometimes not created to the ideal aesthetic and functional scheme. When improperly fabricated, dentures can make an individual appear almost a generation older than their actual age. They can have a poor fit that feels loose and unstable when eating or speaking, and they can actually accelerate bone loss over time.

Salvaging Ms. N’s Severely Broken-Down Upper and Lower Teeth from Gum and Bone Disease
Many people in the U.S. suffer from extensive periodontal disease characterized by significant bone loss and shrinkage of the gum tissue. This condition can begin at a very young age and worsen quickly due to hereditary factors and lack of early diagnosis by their dentist.

Rejuvenating Maria’s Severely Worn Down Implant Overdentures
Many times, per year, patients come to us frustrated because their implant prosthesis is so severely worn down that they are very self-conscious and cover up their smile. They look and feel much older than their age as a result of the extensive wear of their appliance(s).
Replacing a Discolored Front Tooth with a Precision Placed Implant
Some of the most challenging restorations occur when fabricating an anterior crown to fit on an implant. Not only does one have the difficulty of matching the single front tooth to the other ones in the high visibility zone, but the dentist must also ensure the position of the underlying implant is precise through accurate preplanning and placement.
Related Articles
Deepen your knowledge with additional insights on this topic.
 Dental Implants
Dental Implants If a Single Front Tooth is Replaced with an Implant, can it Look Natural?
A single front tooth implant can look completely natural with precision placement, custom abutments, and hand-crafted porcelain crowns. Washington, DC.
 Dental Implants
Dental Implants What is Precision Implant Placement (PIP)?
Learn what Precision Implant Placement (PIP) is and how meticulous planning ensures optimal implant positioning for long-lasting results in Washington, DC.
 Dental Implants
Dental Implants What is the ideal Surgical Guide for Precision Implant Placement?
CBCT-based surgical guides allow virtual implant planning for precise positioning in optimal bone, ensuring predictable results in Washington, DC.
 Dental Implants
Dental Implants When Should an Implant not be Done?
Not every patient is a candidate for dental implants. Learn when healthy roots, fragile bone, or steep angles may make alternatives the better choice.
 Dental Implants
Dental Implants What is Staged Implant Therapy?
Staged implant therapy replaces teeth gradually using existing teeth as temporary support. A personalized alternative to All-on-X for full-arch cases.
Unveiling the Four Types of Dental Implants: Which One's for You?
Learn about the four types of dental implants - endosteal, subperiosteal, zygomatic, and mini implants - and which option may be right for your needs.
Our Services in Potomac
Beyond loose-dental-implant, Potomac patients rely on Dr. Gerald Marlin for a full range of advanced dental care.
More services available in Potomac:
loose-dental-implant Near Potomac
Dr. Gerald Marlin also provides loose-dental-implant services for patients in these neighboring communities.
Getting Here from Potomac
Elite Prosthetic Dentistry is conveniently located near Potomac, MD.
Potomac is accessible via River Road or Darnestown Road. Located north of our main office location.
Address:
4400 Jenifer Street NW, Suite 220
Washington, DC 20015
Phone: (202) 244-2101
Schedule ConsultationSchedule Your Consultation from Potomac
Potomac residents trust Dr. Gerald Marlin for precision dental care. With 3,900+ implants placed and 40+ years of experience, your smile is in expert hands.