
Full Mouth Reconstruction in Washington, DC
Specialist full mouth reconstruction in Washington DC. Dr. Marlin rebuilds failing bites, restorations, and implants at the highest prosthodontic level.
Full Mouth Reconstruction in Washington, DC
Full mouth reconstruction is for patients whose teeth, bite, restorations, or implants are no longer functioning as they should, and for patients who want major restorative treatment planned and executed to a higher standard from the beginning.
Patients from Bethesda, Potomac, Chevy Chase, McLean, Arlington, Fairfax, and surrounding communities come to our Washington, DC office for specialist full mouth reconstruction and bite rehabilitation.
Request a Comprehensive Evaluation Request a Second Opinion Call to Discuss Your Situation
A Systems-Level Approach to Rebuilding the Bite
When multiple teeth, restorations, implants, or bite relationships are involved, the problem usually cannot be solved one tooth at a time.
Full mouth reconstruction evaluates the mouth as a system. That includes bite mechanics, wear, structural support, restorative materials, implant integration where relevant, and the long-term stability of the final result.
Some patients seek this type of care because previous dentistry is breaking down. Others seek it because they want aging dental work replaced or a major treatment plan done correctly the first time. In both situations, the evaluation has to be comprehensive, not piecemeal.
Who Comes for This Type of Care
This type of care is often appropriate for patients with worn, breaking, or repeatedly failing dental work, bite instability, jaw symptoms, collapsing restorations, implant-related complications, or extensive restorative needs.
It is also appropriate for patients who want to replace older crowns, bridges, veneers, or prior reconstruction with a more stable long-term solution, and for patients who want a specialist evaluation before moving forward with major treatment.
While Elite Prosthetic Dentistry provides a refined version of All-on-X therapy — including All-on-4® and All-on-6® — where it is clinically appropriate, the practice preferentially preserves natural teeth wherever doing so produces a stronger long-term result. The decision is made case by case based on diagnosis, not preference.
Why Patients Choose a Prosthodontist for Full Mouth Reconstruction
Full mouth reconstruction requires more than isolated procedures. It requires diagnosis, sequencing, restorative design, and control over how the bite and aesthetics work together over time.
That is why many patients seek a prosthodontist when treatment becomes more complex, when previous dentistry has not held up, or when they want a more precise long-term solution rather than repeated patchwork.
What Is Full Mouth Reconstruction by Salvaging Your Teeth?
Full mouth restoration in Washington, DC, blends the art and science of restorative and cosmetic procedures to restore oral function while secondarily improving your smile appearance. Our prosthodontist has in-depth knowledge of facial anatomy and oral structures and 40 years of experience in delivering transformative restorative procedures. Our on-site dental lab enhances his ability to design exceptionally well-crafted restorations that provide harmonious, natural-looking results.

Issues Treated with Full Mouth Reconstruction
- Extensive gum disease and/or dental decay
- Multiple failing or missing teeth
- Severely worn or broken teeth due to teeth grinding and clenching
- Jaw pain and TMJ disorder from a misaligned bite
- Dental trauma including broken or knocked-out teeth


The Art and Science of Full Mouth Restoration
At your initial consultation, our prosthodontist will discuss your current oral health issues and smile goals, perform an oral exam, and use advanced digital technology to make an accurate diagnosis and plan treatment. The next step is helping you decide on the most optimal procedures to restore your unique set of problems. At Elite Prosthetic Dentistry, we frequently stage dental reconstruction in Washington, DC, in phases to ensure proper healing, patient comfort, integration of restorations between procedures, and excellent results. The process may require additional procedures and a more extended treatment timeline if you have significant dental issues, such as widespread tooth loss, severe decay, or advanced gum disease.
The Benefits of Full Mouth Reconstruction
- Better chewing and a more comfortable bite
- Protection from future tooth damage
- Restored ability to speak clearly
- Improved gum health
- Enhanced confidence and quality of life
- Beautiful smile aesthetics
The Proof Is In Our Patients






What the Evaluation Is Designed to Clarify
The consultation is designed to determine what is causing the breakdown, what can be preserved, what needs to be replaced, and what a stable, long-term result should involve. This is not a quick cosmetic opinion. It is a prosthodontic evaluation of the full system.
Request a Comprehensive Evaluation Call to Discuss Your Situation
Full Mouth Reconstruction Procedures
Dental Crowns & Bridges
Patients who seek our expert care often receive crowns or bridges elsewhere that have already been replaced one or more times. Although we provide milled, ceramic-based crowns where appropriate, we usually merge the best digital technology with hand-crafting expertise, providing an ideal fit with a dazzling smile. Learn more about our custom-crafted crowns and bridges.
All our crowns and bridges are masterfully fabricated at our on-site dental lab with different porcelains on either an all-ceramic or high noble metal base (coping). Our highly skilled in-house technician fabricates crowns and bridges with the utmost precision and attention to detail, delivering restorations that typically last 35 years or longer!
Dental Implants
If your teeth are too severely decayed, damaged, or diseased to save, implant specialist in Washington DC are an excellent long-term investment because they replicate your natural teeth’ appearance, function, and durability. After they fuse with your underlying jawbone, dental implants prevent bone loss and changes to your facial structure, restore 99% of oral function, and offer exceptional longevity. That said, getting dental implants from a highly skilled implant surgeon is essential.
Precision Implant Placement
Creating great smiles with dental implants is a highly sophisticated process that presents challenges. Every aspect of the dental implant process, from planning and surgical insertion to the placement of the final restoration, requires in-depth skills to achieve the highest levels of precision placement and restoration. At Elite Prosthetic Dentistry, we rely on cutting-edge technology and decades of expertise to eliminate guesswork and provide a radiant, natural smile built on a stable, strong foundation topped with beautiful restorations crafted on-site.
Front Tooth Replacement
Missing a front tooth in your smile zone can cause embarrassment and damage self-esteem. Replacing a front tooth with a dental implant and crown is one of the most challenging areas of restorative dentistry, especially when it involves one of the two central incisors in the midline. Our prosthodontist goes above and beyond to deliver outstanding front tooth replacement. This includes advanced imaging to analyze your bone health and formulate a precise surgical plan and create guides, precision dental implant placement, internal coloration for a 3D effect, and custom chairside staining of your crown to match adjacent teeth.
Implant-Restored Fixed Bridge
Although a traditional bridge is a cost-effective dental reconstruction, healthy anchor teeth must be modified and crowned, and bone loss continues under the false tooth or teeth. Our fixed implant bridges rely exclusively on dental implants to support your prosthesis, preserving your underlying jawbone while providing more excellent function and aesthetics. With advanced dental technology, meticulous surgical planning, and decades of top-level expertise, you’ll benefit from aesthetically pleasing, highly durable implant-supported bridges created at our on-site dental lab.
Ridge Augmentation & Bone Grafting
Whether you have bone deterioration due to tooth loss, gum disease, or trauma, various bone grafting procedures at Elite Prosthetic Dentistry can resolve this problem and allow you to receive restorative dental procedures. If you have existing bone loss and require dental implants, bone grafting is often necessary to ensure proper fusion with your underlying jaw bone.
Ridge augmentation is a procedure that adds bone graft material to the outside of the ridge bone that surrounds your teeth. Special drills expand the ridge internally with bone added in the newly formed “tooth” socket. The sites are protected with a special barrier membrane and allowed to heal and integrate before precision implant placement in Washington, DC.
Failing Implant Repair
Dental implants can fail for a number of reasons, from untreated periodontal disease to imprecise placement or restoration. Dr. Marlin is widely referred for repairing failing dental implants and maintains a documented in-practice success rate exceeding 97% on implants placed more than 20 years ago. His patented implant restoration system has been used to restore more than 14,000 dental implants and is particularly useful where prior implants were placed at unfavorable angles or rotations.
Mini Dental Implants
Mini dental implants are fabricated from the same biocompatible materials as standard dental implants but with a reduced diameter (less than 3 mm) and a shorter length. Because they’re more minor and less permanent, mini dental implants often provide immediate anchorage for overdentures. Mini dental implants aren’t as strong or long-lasting as regular implants. Therefore, they should be replaced within several months to one year.
The Full Spectrum of Reconstructive Services
A full mouth reconstruction may incorporate many specialized procedures depending on your needs. Sinus augmentation and ridge augmentation rebuild bone volume for implant support. Porcelain veneers and teeth whitening address cosmetic concerns in the smile zone. For patients with TMJ dysfunction, bite correction is integrated into the overall reconstruction plan. All prosthetic components are designed with CAD/CAM technology and fabricated in our in-house laboratory.
When a Specialist Evaluation Is the Right Next Step
If you are considering full mouth reconstruction, replacing older dental work, or trying to understand why previous treatment is not holding up, a specialist evaluation can provide clarity.
Request a Comprehensive Evaluation Call to Discuss Your Situation
No pressure. Clear answers. A defined plan.
Serving Patients From
Maryland
Bethesda (Advanced Restorative Dentistry) | Bethesda (Dental Fillings) | Bethesda (Full Mouth Reconstruction) | Cabin John | Chevy Chase | Kensington | North Bethesda | Potomac | Rockville | Silver Spring
Washington, DC
Cleveland Park | Dupont Circle | Foxhall | Georgetown | Kalorama | Palisades | Spring Valley | Tenleytown | Woodley Park
Virginia
Your Best Smile Is Within Reach
Request a specialist consultation with Dr. Marlin to discuss your situation and the most appropriate path forward.
Frequently Asked Questions
What is full mouth reconstruction and who needs it?
Full mouth reconstruction is a comprehensive treatment plan that combines restorative and cosmetic procedures to rebuild an entire smile. It is recommended for patients dealing with extensive decay, failing or missing teeth, severe wear from grinding, advanced gum disease, TMJ disorders, or dental trauma that affects multiple teeth.
How long does a full mouth reconstruction take?
Treatment duration depends on the complexity of the case and the procedures involved. Some patients complete treatment in several months, while more complex cases involving bone grafting, implant placement, and custom crown fabrication may take a year or longer. Dr. Marlin develops a detailed treatment timeline during your initial consultation.
What procedures are included in a full mouth reconstruction?
A full mouth reconstruction may include dental crowns and bridges, dental implants, precision implant placement, front tooth replacement, implant-restored fixed bridges, ridge augmentation, bone grafting, failing implant repair, and mini dental implants. The specific combination of procedures is customized to each patient's needs.
How long do full mouth reconstruction results last?
With proper care, the results of full mouth reconstruction can last decades. Crowns and bridges fabricated in the in-house lab at Elite Prosthetic Dentistry have demonstrated longevity of 35 years or more. Dental implants placed by Dr. Marlin show a 97% success rate after 20 years.
Can full mouth reconstruction help if other dentists said my case is too complex?
Yes. Dr. Marlin specializes in complex cases that other dentists may not have the training or experience to handle. With 40 years of experience in periodontal prosthesis and implant therapy, he regularly treats patients who have been told their cases are too difficult or that their teeth cannot be saved.
Related Patient Success Stories
Explore similar patient success stories demonstrating our expertise in advanced prosthetic dentistry.
 Before
Before  After
After How Aging, Opaque Restorations Were Replaced with Customized Ceramic Restorations Designed for Long-Term Natural Esthetics
The existing restorations appeared opaque, worn, and unnatural over time, affecting both confidence and overall smile harmony.
 Before
Before  After
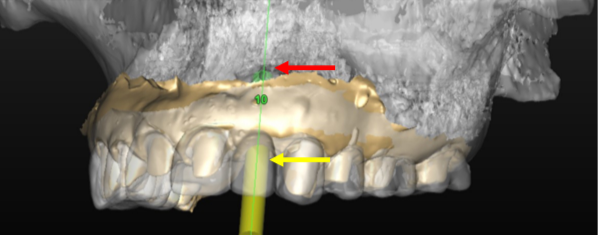
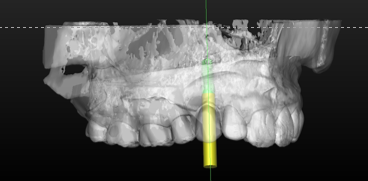
After How Older Implant Crowns Were Redesigned for a Better Bite and More Natural Appearance
The patient came in after years of living with implant-supported crowns placed more than twenty years earlier that no longer looked or functioned well. CBCT evaluation, reviewed with a radiologist colleague, showed the implants had been placed too far to the buccal in very thin bone and could not support a healthy long-term restoration.
 Before
Before  After
After How a Front Tooth Lost to Childhood Trauma Was Rebuilt with Bone Grafting and a Long-Lasting Implant
A teenager was referred by her father after earlier trauma left her upper left front tooth slowly failing from root resorption. She was still growing, so an immediate implant was the wrong move. The tooth had to be maintained to buy time, then replaced correctly once she reached skeletal maturity.
 Before
Before  After
After Two Front Teeth Saved From Extraction: A Second Opinion, Custom Gold Posts, and Crowns Made to Last
Two upper central incisors with failed root canal treatment and recurrent decay had been recommended for extraction and implant replacement. A CBCT evaluation showed that removing the roots from their thin facial bone housing could create a visible esthetic defect in the gum and bone contour, made worse by the patient's high lip line.
 Before
Before  After
After How Severe Bone Loss and Bite Dysfunction Were Rebuilt with All-on-6 Implants and a Milled Zirconia Hybrid Prosthesis
The patient presented with severe bone loss, advanced periodontal disease, malocclusion, and a dysfunctional bite that required full-arch rebuilding.
 Before
Before  After
After Implant Supported Reconstruction: Failing Bridgework and Missing Back Teeth Rebuilt with Coordinated Specialist Care
Referred by another dental specialist with severe bone resorption on the upper left, multiple broken-down lower teeth requiring extraction, and failing lower back teeth that had left the bite without solid support. No single procedure, and no single provider working alone, could rebuild a situation this interconnected.
Related Articles
Deepen your knowledge with additional insights on this topic.
 Dental Implants
Dental Implants If a Single Front Tooth Is Replaced with an Implant, Can It Look Natural?
Yes. See the four steps, with real case photos, that make a single front tooth implant indistinguishable from the natural tooth beside it. Washington, DC.
 Dental Implants
Dental Implants What Is Precision Implant Placement (PIP)?
Precision Implant Placement plans each implant virtually on a CBCT scan, then delivers it with a custom surgical guide. See the three steps with real images.
 Dental Implants
Dental Implants What Is the Ideal Surgical Guide for Precision Implant Placement?
Not all surgical guides are equal. The gold standard is CBCT-based: planned virtually in 3D, 3D printed, and seated on your teeth. A DC prosthodontist explains.
 Dental Implants
Dental Implants When Should an Implant Not Be Done?
Healthy roots, thin bone, steep bony angles: a DC prosthodontist shows a real case where refusing implants was the right call, and what was done instead.
 Dental Implants
Dental Implants What Is Staged Implant Therapy?
Staged implant therapy replaces failing teeth in phases while you keep fixed teeth the entire time. A DC prosthodontist walks through a real case in stages.
Dental Implants The Four Types of Dental Implants: Which One Is Right for You?
Endosteal, subperiosteal, zygomatic, and mini implants each solve a different problem. A DC prosthodontist explains the four types and who each one fits.
Ready to Transform Your Smile?
With 40+ years of experience and 3,900+ dental implants placed and restored, Dr. Marlin delivers results that last. Request a specialist consultation.